The question of how to manage external hemorrhoids effectively, safely, and with minimal risk of recurrence remains a major concern for a large proportion of affected individuals. The following article provides a comprehensive and evidence-based overview to address this issue in detail.
What are external hemorrhoids?
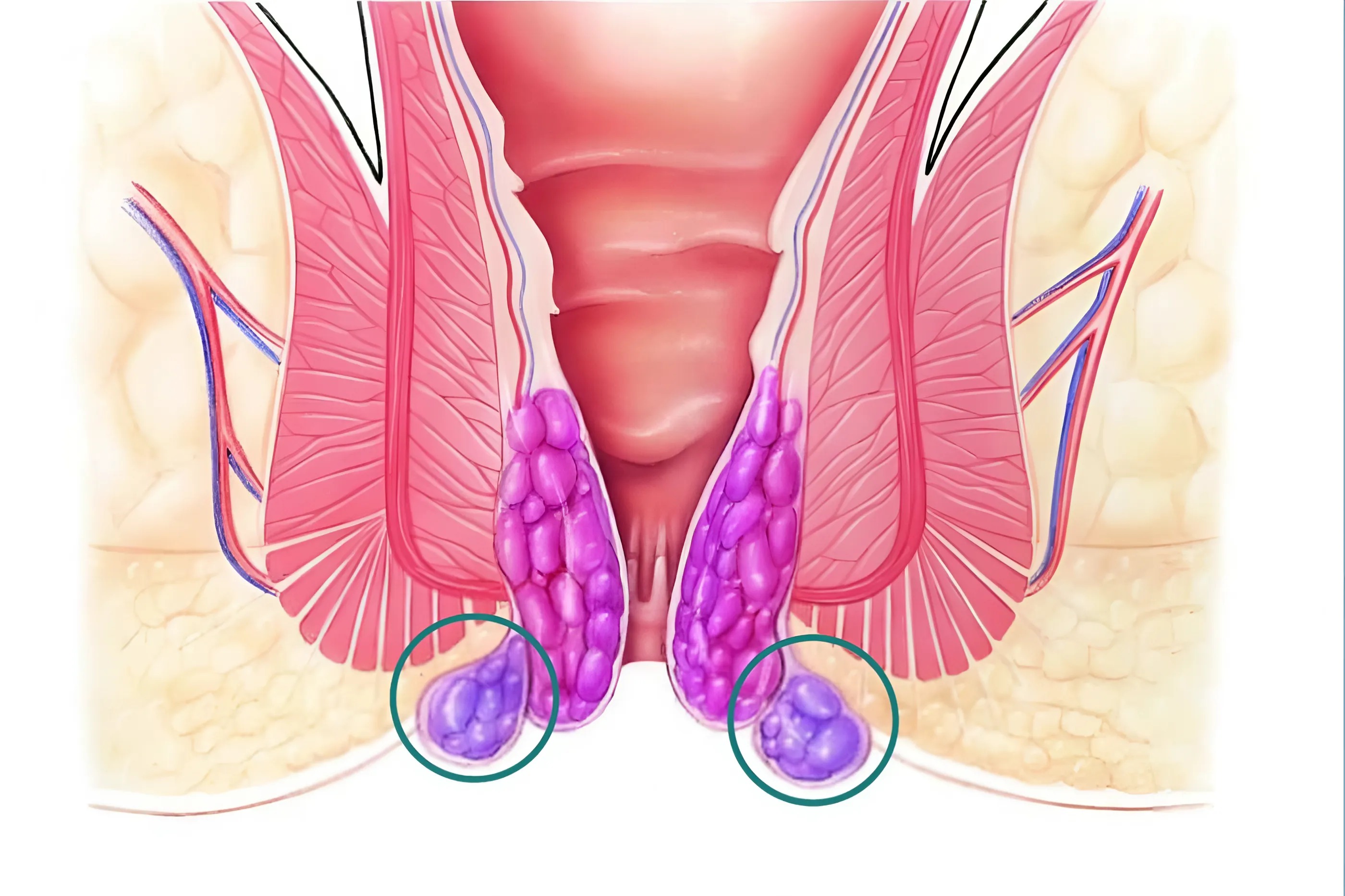
External hemorrhoids are characterized by venous dysfunction at the anal verge, leading to abnormal dilatation and engorgement of the perianal venous plexus, ultimately forming hemorrhoidal masses. In contrast to internal hemorrhoids, which arise within the anal canal above the dentate line, external hemorrhoids develop outside the anal canal beneath the perianal skin.
In the early stages, hemorrhoidal nodules are typically small, often comparable in size to a pea. However, in the absence of appropriate and timely management, these lesions may progressively enlarge, evolving into prominent masses that cause significant discomfort, pruritus, and a burning or painful sensation in the perianal region.
In more advanced or severe cases, patients may experience intensified pain, particularly when sitting, and may also develop bleeding. At this stage, surgical intervention, including hemorrhoidectomy, may be indicated for definitive management.
Clinical manifestations of external hemorrhoids
The clinical presentation of external hemorrhoids varies depending on the stage and severity of disease progression. Common signs and symptoms may include:
Mild external hemorrhoids
In the early stages, patients may present with the following clinical features: Fresh bright red rectal bleeding, typically noted during defecation. A persistent sensation of incomplete evacuation or tenesmus, accompanied by a feeling of pressure in the anal region. Anal pain and burning, occurring during and after bowel movements, or presenting as a persistent dull discomfort throughout the day, particularly exacerbated by prolonged sitting.Prolapse of hemorrhoidal tissue outside the anal verge following defecation. Pruritus affecting the perianal or rectal area.
Severe external hemorrhoids
In advanced stages, symptoms become more pronounced and may include: The presence of perianal tissue resembling skin tags or soft masses, often erythematous and highly vascularized. A persistent burning sensation in the anal region. Marked enlargement of hemorrhoidal masses, frequently exhibiting a bluish purple discoloration. Thrombosed external hemorrhoids, associated with significant pain and a high risk of rupture upon friction or mechanical irritation.
Common and predisposing factors associated with hemorrhoidal disease
The exact etiology of hemorrhoidal disease has not been fully elucidated. However, it is widely recognized that hemorrhoids are more likely to develop in individuals with predisposing factors that increase intra rectal pressure and exert mechanical stress on the anorectal venous system. This leads to impaired venous return, venous stasis, and subsequent dilation of the hemorrhoidal plexus, resulting in the formation of hemorrhoidal masses.
Several common risk factors contributing to the development of hemorrhoids include:
- Unhealthy dietary habits: An imbalanced diet, including excessive alcohol consumption, frequent intake of fast food, and inadequate nutritional composition, is a major contributing factor. Notably, a low fiber diet is considered one of the leading causes of hemorrhoidal disease, as it results in hard stools and difficulty during defecation.
- Sedentary lifestyle and prolonged sitting: Individuals with occupations that require prolonged sitting or maintaining a fixed posture, such as office workers, factory workers, tailors, and drivers, are at increased risk. Additionally, frequent heavy lifting may further exacerbate the condition. Prolonged pressure on the anorectal region impairs venous return, leading to venous dilation and the formation of hemorrhoidal masses.
- Chronic constipation or diarrhea: Persistent bowel habit disturbances, including chronic constipation or prolonged diarrhea, significantly increase the risk of hemorrhoid development due to repeated straining or irritation of the anorectal mucosa.
Constipation and hemorrhoidal disease are closely interrelated. In patients with hemorrhoids, defecation is often associated with pain, burning, and significant discomfort. Many individuals tend to avoid or delay bowel movements due to fear that defecation may exacerbate their condition or intensify pain. This behavior can lead to constipation or further aggravate existing constipation.
Chronic constipation or persistent diarrhea increases intestinal motility and straining, thereby exerting excessive pressure on the venous system of the anus and rectum, ultimately contributing to the development or progression of hemorrhoids.
Reader may also be interested in:
- Stages of external hemorrhoids – when should you seek medical care?
- Signs of external hemorrhoids – when should you seek medical attention?
- Etiology of external hemorrhoids and effective preventive strategies
In addition, several other contributing factors may elevate the risk of hemorrhoidal disease, including pregnancy, obesity, and chronic psychological stress or fatigue.
Stages of external hemorrhoids
External hemorrhoids typically develop and progress through four clinical stages, with a gradual increase in severity over time.
- Stage 1: Hemorrhoidal tissue begins to form, typically without overt clinical symptoms.
- Stage 2: Progressive enlargement of the hemorrhoidal mass, with protrusion beyond the anal verge, leading to discomfort and a sensation of obstruction.
- Stage 3: Further enlargement is accompanied by vascular complications, including thrombosis, resulting in significant pain and possible bleeding.
- Stage 4: Advanced disease characterized by marked inflammation, severe pain, and swelling, with a high risk of complications, substantially impairing overall health status and daily functioning.
For patients with mild external hemorrhoids (Stage 1 and Stage 2), when hemorrhoidal masses are newly formed and clinical symptoms remain minimal or absent, conservative management is typically the first line of treatment. This approach includes pharmacological therapy combined with appropriate dietary modifications and the adoption of a healthy lifestyle.
In cases where external hemorrhoids have progressed to more advanced stages (Stage 3 and Stage 4), the hemorrhoidal masses are significantly enlarged, accompanied by severe symptoms and an increased risk of complications such as infection, thrombosed external hemorrhoids, or tissue necrosis. In these situations, procedural or surgical intervention, including hemorrhoidectomy, is often indicated for definitive treatment.
These observations highlight the importance of early medical evaluation and timely diagnosis. When external hemorrhoids are managed at an early stage with appropriate therapeutic strategies, treatment tends to be less invasive, associated with reduced pain, higher clinical efficacy, and a substantially lower risk of recurrence.
Stage based management of external hemorrhoids
Management of Stage 1 and Stage 2 external hemorrhoids
In patients with early stage external hemorrhoids, conservative treatment is the preferred approach, consisting of pharmacological therapy in combination with dietary and lifestyle modifications. At this stage, when hemorrhoidal masses are newly formed, medical therapy is effective in alleviating symptoms and preventing disease progression.
In clinical practice, patients are commonly prescribed a combination of oral medications and topical agents to achieve optimal therapeutic outcomes. Frequently used medications include:
- Analgesics for pain relief and symptomatic control.
- Anti inflammatory agents to reduce edema and local inflammation.
- Laxatives to facilitate bowel movements.
- Stool softeners to decrease straining during defecation.
- Venoactive drugs to enhance venous tone and improve vascular integrity.

Patients should be advised that the choice of medication and dosage must be prescribed by a qualified physician following a thorough clinical evaluation, including assessment of disease severity and symptom burden.
In addition to pharmacological therapy, patients are strongly encouraged to adopt an appropriate diet and maintain a healthy lifestyle. Particular attention should be paid to proper daily hygiene of the perianal region, specifically:
- Increase intake of fiber rich foods, including fruits, vegetables, and whole grains.
- Incorporate collagen rich foods such as salmon, tuna, and seaweed.
- Maintain adequate daily hydration by drinking sufficient amounts of water.
- Engage in regular physical activity, with emphasis on light exercises such as walking, swimming, or gentle aerobic practices.
- Avoid prolonged sitting or standing; it is advisable to take short breaks and move around after every hour of sitting.
- Use a donut cushion when prolonged sitting is required to reduce pressure on the anorectal region.
- Establish a regular bowel habit by defecating at a consistent time each day to promote optimal gastrointestinal function and prevent constipation.
- Maintain proper perianal hygiene after defecation by using wet wipes or soft cotton pads to minimize mechanical irritation.
Management of Stage 3 and Stage 4 external hemorrhoids
Although several interventional techniques are available for hemorrhoidal disease, such as sclerotherapy, cauterization, and rubber band ligation, these approaches are generally not preferred for external hemorrhoids. This is primarily due to the high density of sensory innervation in the perianal region, which makes such procedures significantly more painful for patients.
Moreover, these interventions may be associated with potential complications, including bleeding and infection, and are also linked to relatively high recurrence rates in cases of external hemorrhoids.
Therefore, surgical management, particularly hemorrhoidectomy, is widely recommended by clinicians as the definitive treatment for patients with advanced external hemorrhoids.
Common surgical techniques for external hemorrhoidectomy
Several surgical approaches may be considered in the management of external hemorrhoids, including:
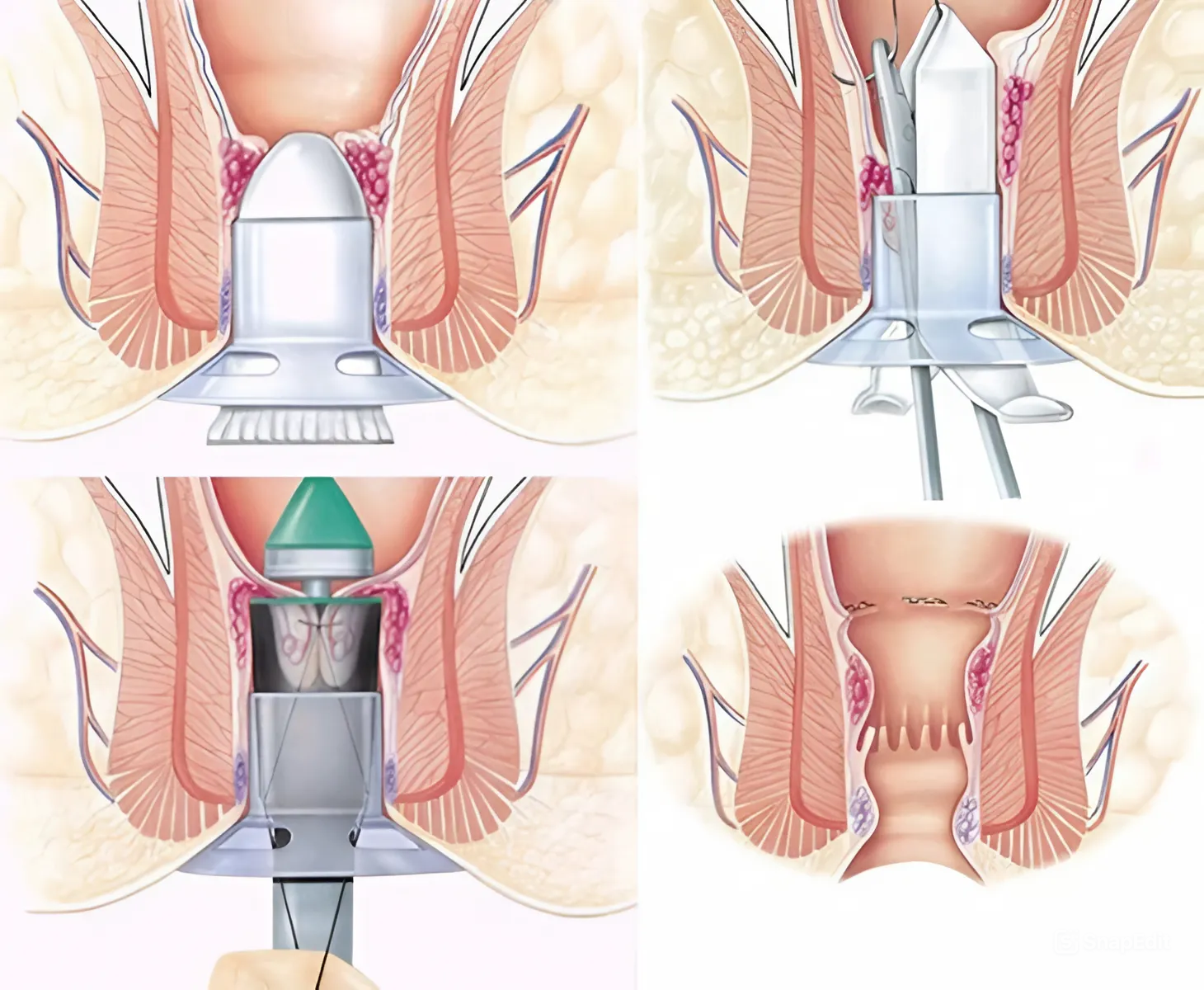
- Longo technique (stapled hemorrhoidopexy): This method utilizes a circular stapling device to reposition prolapsed hemorrhoidal tissue back to its anatomical location. Concurrently, the arterial blood supply to the hemorrhoidal plexus is interrupted, resulting in gradual shrinkage and eventual regression of the hemorrhoidal tissue.
- Milligan Morgan technique: This is a conventional excisional hemorrhoidectomy in which the hemorrhoidal masses are surgically removed. The surgeon then reconstructs the mucocutaneous layer to minimize trauma to the anal canal and promote optimal wound healing.
- PPH technique (Procedure for Prolapse and Hemorrhoids)This technique employs a stapling device inserted into the rectal mucosa to excise redundant tissue and reduce prolapsed hemorrhoids, thereby restoring normal anatomy.
- HCPT technique (High frequency coagulation therapy): This method uses high frequency energy at temperatures ranging from 70 to 80 degrees Celsius to coagulate the blood vessels supplying the hemorrhoidal tissue. Following vascular control, the hemorrhoidal masses are excised.
- Laser hemorrhoidectomy: This technique utilizes high energy lasers with a wavelength of approximately 1470 nm to target the hemorrhoidal plexus at its origin, effectively ablating the feeding vessels. This induces fibrosis and rapid shrinkage of the hemorrhoidal tissue.
Surgical management of external hemorrhoids allows for complete excision of hemorrhoidal masses, offering near definitive therapeutic outcomes with a low risk of recurrence.
However, the selection of an appropriate surgical technique should be determined by a qualified specialist, based on a comprehensive clinical assessment of the patient’s condition. Therefore, prior to undergoing hemorrhoidectomy, patients are strongly advised to seek evaluation from experienced colorectal specialists at reputable healthcare institutions.
It is not recommended to pursue treatment at unregulated or low standard medical facilities, as this may increase the risk of serious complications.
Where to receive effective and reliable treatment for external hemorrhoids?
The Center for Gastrointestinal Surgery, Colorectal and Perineal Surgery at Hong Ngoc General Hospital is recognized as a reputable medical facility for the management of external hemorrhoids, and is widely trusted by a large number of patients.
The center has successfully treated numerous cases of advanced external hemorrhoids (Stage 3 and Stage 4), including those with complications, through:
- Direct consultation with a team of leading colorectal and anorectal specialists, including:
- Associate Professor, PhD, Distinguished Physician Nguyen Xuan Hung, former Director of the Colorectal and Perineal Surgery Center at Viet Duc University Hospital, Vice President of the Vietnam Society of Colorectal and Anal Diseases, and member of the French Society of Coloproctology; Distinguished Physician, PhD, Specialist Level II Pham Van Cuong, with nearly 40 years of clinical experience and member of the Vietnam Society of Endoscopic and General Surgery; Master of Medicine, MD Cu Trung Kien, extensively trained in gastrointestinal surgery in Hong Kong, former physician at Bach Mai Hospital, currently Deputy Head of the Department of Gastrointestinal Surgery at Hong Ngoc General Hospital; Specialist Level I Bach Phuc Huy, with over 15 years of experience, Head of the Gastrointestinal Surgery Unit at Hong Ngoc General Hospital, among others.
- Application of advanced surgical techniques, notably Laser Hemorrhoidoplasty using LHP technology from Germany, performed without conventional scalpel incision and associated with minimal postoperative pain. High energy laser at a wavelength of 1470 nm precisely targets the hemorrhoidal plexus at its origin, effectively obliterating the feeding vessels, thereby inducing rapid fibrosis and shrinkage of hemorrhoidal tissue while preserving surrounding healthy structures.
- Safe and minimally painful surgical outcomes are achieved through a comprehensive perioperative pain management protocol, developed by Master of Medicine, MD Nguyen Thi Thu Ba, who received advanced clinical training in France. The anesthesiology team closely monitors patients throughout the entire surgical procedure.
- A proactive and safe pain prevention strategy is implemented, including thorough pre anesthetic assessment, continuous intraoperative monitoring, and early pain control before symptom onset.
- Comprehensive 24/7 patient care services are provided throughout hospitalization.
- Inpatient facilities are designed to be spacious, hygienic, and fully equipped with amenities comparable to high standard hospitality services.

For further consultation, please contact:
Hotline for specialist appointment scheduling: 0911 908 856Hotline for hemorrhoid surgery consultation: 0949 646 556
Note: The information provided in this article by Hong Ngoc General Hospital is intended for reference purposes only and does not replace professional medical diagnosis or treatment. Patients are strongly advised not to self medicate. For an accurate diagnosis and appropriate treatment plan, individuals should seek direct evaluation and consultation from qualified healthcare professionals at accredited medical facilities.
Follow the official fanpage of Hong Ngoc General Hospital to stay updated with valuable health information and exclusive healthcare promotions.