Esophageal spasm is a common motility disorder characterized by dysphagia, retrosternal pain, and chest tightness, which can be easily mistaken for gastroesophageal reflux disease or cardiovascular conditions. Although the disease often progresses insidiously, failure to achieve accurate diagnosis and appropriate management may significantly impair nutritional intake and overall quality of life.
What is esophageal spasm? Types of esophageal spasm
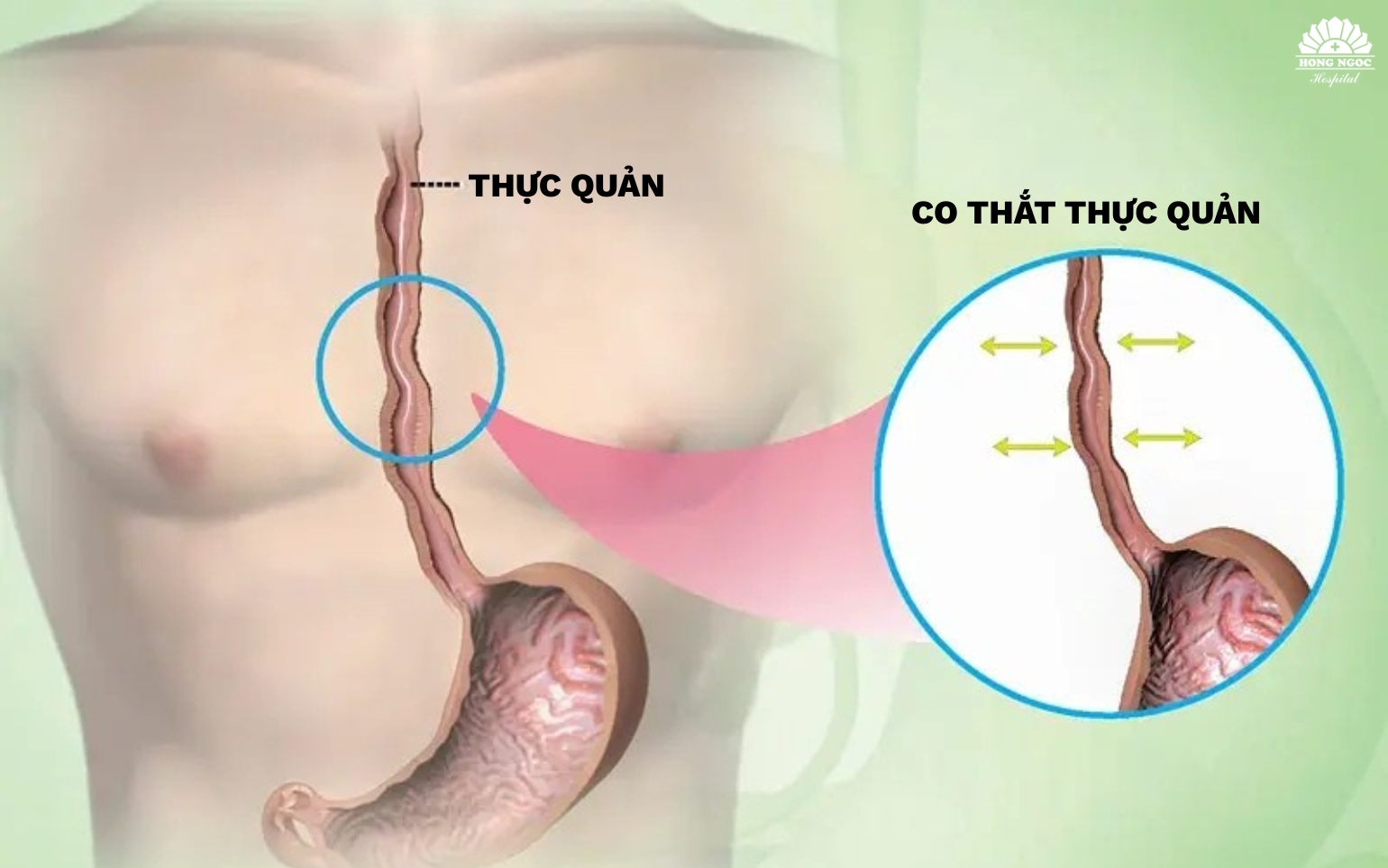
What is esophageal spasm?
Esophageal spasm is a motility disorder of the esophageal smooth muscle, characterized by abnormal, uncoordinated, or excessively forceful contractions that interfere with the normal transit of food from the oropharynx to the stomach.
This is considered a functional esophageal disorder rather than a structural abnormality; however, if not appropriately recognized and monitored, it may significantly impact swallowing function and nutritional intake.
Types of esophageal spasm
Based on esophageal contractility characteristics, esophageal spasm is classified into two main types:
- Distal esophageal spasm: Characterized by uncoordinated contractions predominantly occurring in the distal esophagus near the stomach, leading to chest discomfort, retrosternal pain, and dysphagia. Symptoms are often triggered or exacerbated by eating or psychological stress.
- Hypercontractile esophagus: Involves excessively forceful contractions along the entire esophagus, resulting in dysphagia and significant discomfort during swallowing, which can markedly impact daily activities and quality of life.
What causes esophageal spasm? Who is at risk?
What causes esophageal spasm?
The exact cause of esophageal spasm remains incompletely understood. However, current evidence suggests that it is associated with abnormalities in esophageal motility and impaired neural regulation of esophageal smooth muscle, along with several contributing risk factors, including:
- Esophageal neural dysfunction: Abnormal regulation of the enteric nervous system leads to uncoordinated esophageal contractions.
- Gastroesophageal reflux disease (GERD): Chronic acid exposure irritates the esophageal mucosa, increasing the risk of motility disturbances.
- Psychological stress: Prolonged anxiety and stress can disrupt the brain gut axis, contributing to impaired esophageal motility.
- Dietary factors: Consumption of very hot or cold foods, as well as alcohol (particularly red wine), may trigger esophageal spasm.
- Esophageal inflammation or infection: Inadequately treated inflammation may result in structural and functional abnormalities.
- Thoracic or cervical medical interventions: Procedures such as radiotherapy or esophageal surgery may damage neural pathways controlling esophageal function.
- Genetic predisposition: A family history of esophageal disorders may increase susceptibility.
- Associated medical conditions: Autoimmune diseases, chronic inflammation, fibrosis, or esophageal strictures may contribute to underlying pathophysiology.
Accurate identification of the underlying cause of esophageal spasm is essential for selecting appropriate therapeutic strategies, thereby improving symptom control and preventing long term complications.
Who is at risk of esophageal spasm?
Esophageal spasm can occur across various age groups; however, it is more commonly observed in women and individuals over 60 years of age. In addition to age and sex, several factors may increase the risk, including:
- Chronic gastroesophageal reflux disease, leading to persistent irritation of the esophageal mucosa.
- Unhealthy dietary habits, particularly frequent consumption of excessively hot or cold foods and beverages.
- A family history of esophageal motility disorders, suggesting a genetic predisposition.
- Individuals experiencing chronic stress, anxiety, or depression, which may affect neural regulation of esophageal function.
- Frequent symptoms of heartburn or acid regurgitation, indicating underlying esophageal motility dysfunction.
Clinical manifestations of esophageal spasm
Symptoms of esophageal spasm vary among individuals depending on the underlying cause and severity of motility dysfunction. Common clinical features include:
- Dysphagia: A sensation of difficulty swallowing, with food feeling stuck in the throat or behind the sternum.
- Retrosternal chest pain: Often severe, may radiate to the neck, shoulders, or back, and can mimic cardiac chest pain; symptoms may worsen in the supine or lateral position.
- Heartburn and burning sensation: Resulting from associated gastroesophageal reflux, causing discomfort in the chest and throat.
- Regurgitation without nausea: Passive backflow of food or gastric contents into the throat, distinct from vomiting.
- Additional symptoms: May include persistent heartburn, globus sensation, nausea, vomiting, unexplained weight loss, halitosis, chronic cough, and wheezing.

Diagnosis of esophageal spasm
Accurate diagnosis of esophageal spasm is essential to identify underlying motility disorders, guide appropriate treatment, and prevent potential complications. Clinicians typically combine clinical evaluation with paraclinical investigations, including:
Clinical evaluation
- Assessment of characteristic symptoms such as dysphagia, chest pain, globus sensation, heartburn, and regurgitation.
- Evaluation of onset, frequency, and aggravating factors (e.g., stress, dietary triggers).
- Review of medical history, including gastrointestinal, neurological conditions, and associated risk factors.
Paraclinical investigations
- Upper gastrointestinal endoscopy: Direct visualization of the esophageal mucosa to exclude structural lesions.
- Barium esophagography: Identification of abnormal esophageal contractions and motility patterns.
- Esophageal manometry: Gold standard test to evaluate esophageal motility and characterize contraction patterns.
- 24 hour esophageal pH monitoring: Helps differentiate esophageal spasm from gastroesophageal reflux disease.
The Gastroenterology Center at Hong Ngoc General Hospital brings together highly experienced specialists and is equipped with advanced endoscopic and diagnostic systems, enabling accurate detection of esophageal spasm and effective differentiation from esophageal malignancy.
For detailed consultation, please contact the hotline at 0911 908 856.
Complications of esophageal spasm
If not promptly diagnosed and appropriately managed, esophageal spasm may lead to several complications that adversely affect health and quality of life, including:
- Chronic dysphagia: Impaired esophageal transit results in poor oral intake, leading to weight loss and malnutrition.
- Recurrent chest pain: Episodes of severe chest pain may mimic cardiovascular disease, causing persistent anxiety and reduced quality of life.
- Gastroesophageal reflux disease (GERD): Disordered esophageal motility may predispose to acid reflux and subsequent esophagitis.
- Esophagitis, ulceration, or stricture formation: Chronic irritation and inflammation can damage the esophageal mucosa, worsening dysphagia.
- Generalized physical debilitation: Prolonged nutritional impairment may result in dehydration, fatigue, and decreased immune function.
Management of esophageal spasm
As the exact etiology of esophageal spasm remains unclear, current treatment strategies primarily focus on symptom relief and prevention of complications. Depending on the severity of symptoms and the degree of impact on daily activities, management is typically categorized into three main approaches:
Lifestyle and dietary modifications
- Avoid extremely hot or cold foods and beverages; limit alcohol, tobacco, and spicy foods.
- Eat slowly, chew thoroughly, and consume smaller, more frequent meals to reduce esophageal stress.
- Maintain psychological well being and minimize stress, as it may exacerbate esophageal spasm.
Pharmacological management
- Smooth muscle relaxants (e.g., calcium channel blockers, nitrates) to reduce esophageal contractions.
- Low dose antidepressants to help alleviate chest pain associated with motility disorders.
- Proton pump inhibitors (PPIs) in cases associated with gastroesophageal reflux disease.
Interventional and surgical treatment
- Endoscopic botulinum toxin injection to provide temporary relaxation of esophageal muscles.
- Endoscopic balloon dilation in cases with significant esophageal narrowing.
- Surgical options such as Heller myotomy or peroral endoscopic myotomy (POEM), which are minimally invasive and effective for severe or refractory cases.
For accurate consultation, diagnosis, and safe management of esophageal spasm, patients are advised to seek care at the Gastroenterology Center of Hong Ngoc General Hospital, where experienced specialists and advanced endoscopic systems enable early detection and effective intervention.

For appointment booking, please contact the hotline at 0911 908 856.
Prevention of esophageal spasm
Although there is no definitive method to completely prevent esophageal spasm, patients can reduce symptoms and minimize the risk of complications through the following measures:
- Dietary modification: Consume smaller, more frequent meals; prioritize soft, easily digestible foods; and increase dietary fiber intake.
- Avoid esophageal irritants: Limit very hot or cold foods, spicy and high fat meals; avoid alcohol, caffeinated beverages, and tobacco.
- Adopt proper eating habits: Eat slowly, chew thoroughly, and avoid lying down immediately after meals.
- Maintain a healthy lifestyle: Manage stress effectively and maintain psychological well being, as chronic stress may exacerbate esophageal motility disorders.
- Regular health check ups: Seek evaluation at reputable healthcare facilities, especially when experiencing symptoms such as persistent dysphagia, chest pain, or heartburn, to enable early diagnosis and timely management.
Frequently asked questions about esophageal spasm
Is esophageal spasm dangerous?
Esophageal spasm is not directly life threatening; however, if persistent and inadequately managed, it may lead to significant complications. These include dysphagia, recurrent chest pain, chronic reflux, malnutrition, and esophageal inflammation or stricture, all of which can markedly impair quality of life. Early evaluation is recommended when symptoms recur.
How can esophageal spasm be relieved?
Management involves a combination of lifestyle modification and medical therapy. Patients are advised to eat slowly, chew thoroughly, avoid extremely hot or cold foods, limit alcohol intake, and reduce stress. Pharmacological treatment or endoscopic interventions should be followed as prescribed to control symptoms and prevent complications.
Can esophageal spasm be cured?
Currently, esophageal spasm cannot be completely cured due to its unclear etiology. However, with early diagnosis and appropriate treatment, symptoms can be effectively controlled, allowing patients to maintain near normal daily activities and reduce long term complications.
When should patients seek medical care?
Patients should consult a physician if they experience persistent or recurrent symptoms such as dysphagia, unexplained chest pain, a sensation of food sticking, or frequent regurgitation. Urgent evaluation is warranted if symptoms worsen, interfere with eating, or are associated with weight loss or significant distress.
How does esophageal spasm differ from GERD?
Although both conditions may present with chest pain and dysphagia, their pathophysiology differs. Esophageal spasm is a motility disorder characterized by abnormal esophageal contractions that impair food transit. In contrast, gastroesophageal reflux disease results from incompetence of the lower esophageal sphincter, allowing gastric acid to reflux into the esophagus, causing heartburn and mucosal inflammation. Diagnostic procedures such as endoscopy and specialized testing are required for accurate differentiation.
Note: The information provided by Hong Ngoc General Hospital is for reference purposes only and does not replace professional medical diagnosis or treatment. For accurate evaluation and appropriate management, patients should seek direct consultation with qualified healthcare providers at reputable medical facilities.
Center for Gastroenterology and Colorectal Disorders – Hong Ngoc General Hospital
- Hong Ngoc Phuc Truong Minh General Hospital – No. 8 Chau Van Liem Street, Nam Tu Liem District, Hanoi
- Hong Ngoc General Hospital – 55 Yen Ninh Street, Ba Dinh District, Hanoi
Hotline: 0911 908 856 – 0932 232 016Email: trungtamtieuhoa@hongngochospital.vn
For more useful health information, please follow the official fanpage of the Gastroenterology Center – Hong Ngoc General Hospital.