Congenital megacolon is a rare congenital anomaly. It is typically identifiable and can be effectively treated; however, delayed diagnosis may lead to serious and potentially life threatening complications.
Megacolon is a condition characterized by abnormal dilation of the colon, leading to reduced intestinal motility. As a result, prolonged transit time allows excessive water reabsorption, causing hard stools and defecation disorders, particularly chronic constipation.
Definition of congenital megacolon
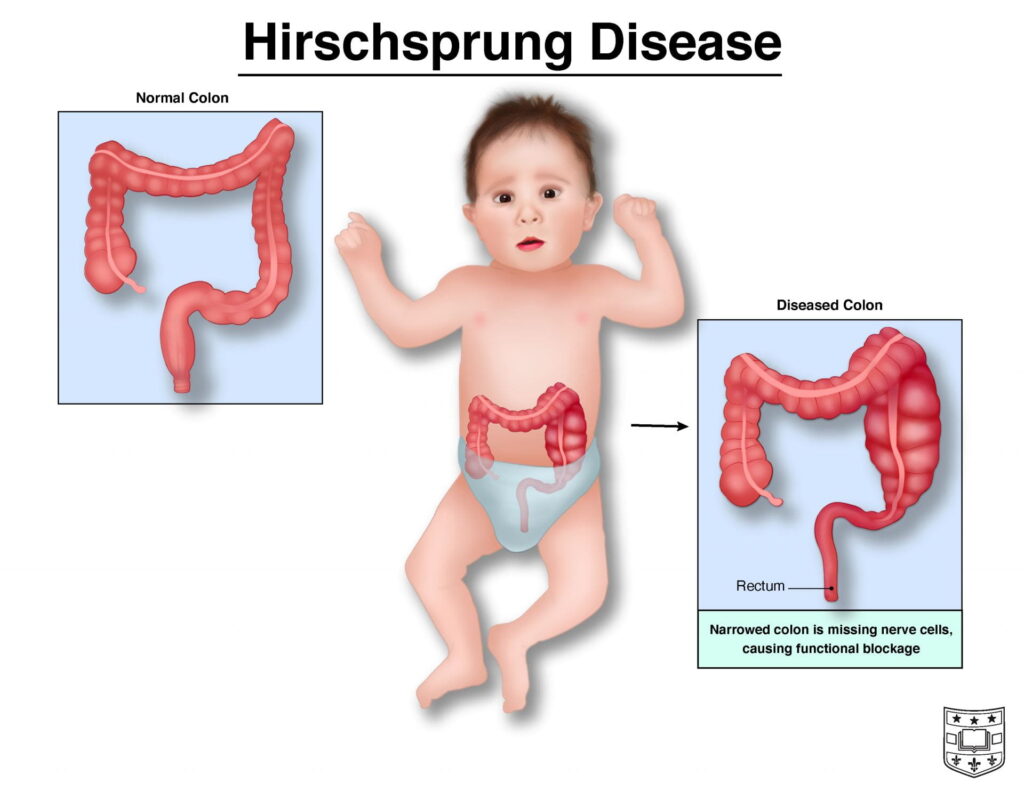
Congenital megacolon, also known as Hirschsprung disease or congenital aganglionic megacolon, is a condition characterized by dilation of the colon due to the absence of enteric ganglion cells in the intestinal wall. This results in functional intestinal obstruction. The segment of bowel proximal to the obstruction becomes progressively dilated, leading to abdominal distension and abnormal bowel movements in affected infants.
This is a congenital disorder with an estimated incidence of approximately 1 in 4,000 to 1 in 5,000 live births. It is more common in males than females, with a male to female ratio ranging from 4:1 to 9:1. Early detection is essential for appropriate monitoring and timely management.
Classification of congenital megacolon
Based on the length of the affected bowel segment, congenital megacolon is classified into four types:
- Short segment disease: Involves only the rectum
- Classic (rectosigmoid) type (approximately 80% of cases): Involves both the rectum and sigmoid colon
- Long segment disease: Extends from the rectum to more proximal segments beyond the sigmoid colon
- Total colonic aganglionosis: Involves the entire colon
Clinical manifestations of congenital megacolon
The clinical presentation of congenital megacolon varies by age and is often recognizable at different developmental stages:
- In neonates: Abdominal distension is a common early sign. Failure to pass meconium within the first 24 hours after birth is a key indicator. Some infants may only pass stool following rectal stimulation, often producing a large volume of feces, known as the “explosive stool” sign. Vomiting may also occur due to intestinal obstruction and abdominal distension.
- In older children: The condition typically presents as chronic constipation lasting for years, alternating with episodes of diarrhea. Stools are often foul smelling and dark due to prolonged fecal stasis. Persistent abdominal distension is common. Affected children may also exhibit malnutrition, poor physical growth, and delayed neurodevelopment.
- Characteristic features: Common signs include severe constipation, dependence on frequent enemas for defecation, abdominal distension, poor appetite, weight loss, and failure to thrive.
It is important to note that not all neonates who fail to pass stool within 24 hours have congenital megacolon. Conditions such as congenital anorectal malformations may present similarly. Regardless of the cause, early diagnosis and prompt surgical management are essential.

Etiology of congenital megacolon
Congenital megacolon results from incomplete development of the gastrointestinal tract during fetal life, particularly due to the absence of ganglion cells within the enteric nervous plexuses located between the muscular layers of the distal intestine. This deficiency leads to loss of normal peristaltic activity, preventing effective bowel motility and defecation.
Under normal conditions, coordinated contractions of intestinal smooth muscle, known as peristalsis, facilitate the movement of intestinal contents. These contractions are regulated by enteric nerves within the bowel wall. In congenital megacolon, the affected bowel segment lacks these nerve cells, rendering it unable to propel stool forward. This functional obstruction causes fecal stasis, while the proximal bowel becomes progressively dilated, leading to abdominal distension.
Additional risk factors for congenital megacolon
Several factors may increase the risk of congenital megacolon, particularly those related to genetic predisposition:
- Familial inheritance: Congenital megacolon may have a hereditary component. If one child in a family is affected, siblings may have an increased risk of developing the condition.
- Male sex: The condition is more commonly observed in males than in females.
- Associated genetic disorders: Congenital megacolon is associated with certain genetic conditions, such as Down syndrome, as well as other congenital anomalies, including congenital heart defects.
Complications of congenital megacolon
Congenital megacolon may be associated with other congenital anomalies, including Down syndrome, cardiovascular disorders, neurological abnormalities, and gastrointestinal or anorectal malformations. Clinical presentation varies depending on disease severity and age at onset.
If left untreated, the condition can lead to long term sequelae such as growth retardation and delayed neurodevelopment.
Affected children often experience poor feeding, resulting in malnutrition and impaired physical and cognitive development. In addition, serious complications may occur, including recurrent enterocolitis, intestinal obstruction, and even bowel perforation.
Therefore, early diagnosis and timely management are essential to minimize complications and improve clinical outcomes.
Management of congenital megacolon
Congenital megacolon requires early diagnosis and prompt treatment. However, many cases are detected late, as symptoms such as constipation or abnormal bowel habits are often misattributed to dietary factors or functional disorders.
When congenital megacolon is suspected, physicians will perform appropriate investigations, including imaging studies. Contrast radiography of the colon plays a key role in diagnosis; however, this technique requires experienced interpretation and should be performed in well equipped medical facilities.
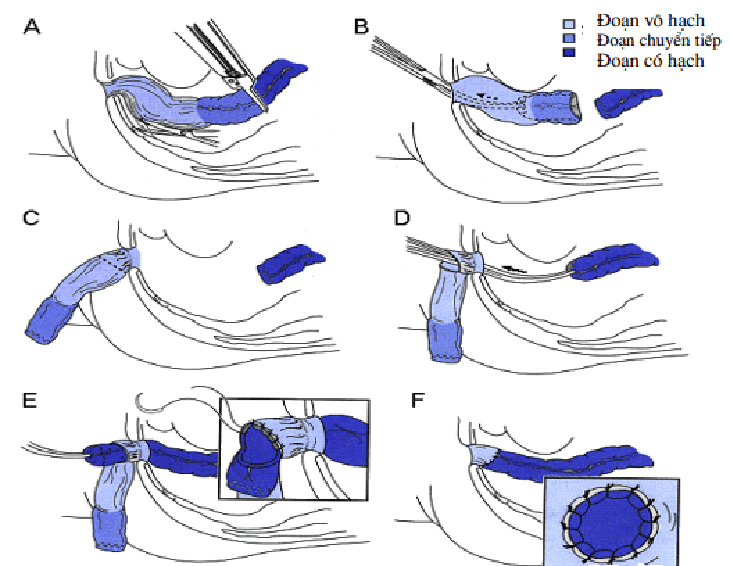
Treatment depends on the underlying pathology and disease severity. The definitive management is surgical, involving resection of the aganglionic segment of the colon followed by pull through and anastomosis with the normal bowel.
In mild cases, conservative management with medications and dietary modification may be considered. In more severe or progressive cases, surgical intervention is indicated. The timing of surgery depends on the stage of diagnosis, severity, and presence of complications.
Surgical techniques have advanced significantly, with options including single stage or multi stage procedures. In most cases today, transanal pull through surgery is preferred, as it is safe, less invasive, and widely applied, often avoiding the need for abdominal surgery.
All confirmed cases in children are indicated for surgical intervention. In recent years, with earlier diagnosis and appropriate preoperative management such as regular rectal irrigation effective single stage surgery can be performed.
The choice of healthcare facility is also a key factor influencing treatment outcomes. Following surgery, the condition can be completely resolved.
Surgical treatment enables children to achieve normal bowel function. This is typically a definitive procedure performed in a single stage via the transanal approach, leaving no visible scars and applicable even in neonates under one month of age.
Postoperatively, infants can usually resume feeding within 1–2 days and may be discharged after approximately one week. In more severe cases, particularly with long segment aganglionosis, laparoscopic abdominal assistance may be required.
In addition, caregivers should encourage a high fiber diet, adequate fluid intake, and regular bowel habits. If a child presents with persistent constipation, especially when associated with abnormal diarrhea, prompt evaluation by a specialist is recommended.
If left untreated, congenital megacolon can significantly impact both physical and neurodevelopmental health. Therefore, early recognition and timely consultation with a pediatric gastroenterology specialist are essential.
Note: The information provided in this article by Hong Ngoc General Hospital is for reference purposes only and does not replace professional medical diagnosis or treatment. Patients should not self medicate. For accurate diagnosis and appropriate treatment planning, individuals are advised to visit a healthcare facility for direct examination, diagnosis, and consultation with qualified physicians.
Follow the official fanpage of Hong Ngoc General Hospital for more health updates and useful information:https://www.facebook.com/BenhvienHongNgoc/
Register for pediatric gastroenterology consultation here: