Accurate grading of internal hemorrhoids is the first and essential step in establishing an effective treatment strategy. Below is a detailed classification of internal hemorrhoids for reference.
What are internal hemorrhoids? Causes of internal hemorrhoids
Internal hemorrhoids are characterized by the abnormal dilation and enlargement of the venous plexus within the anorectal region. In the early stage, hemorrhoidal tissue appears as a small mass located below the dentate line; as the condition progresses, this tissue gradually enlarges and may prolapse outside the anal canal.
Internal hemorrhoids are often difficult to detect in the early stages and can pose challenges in management if not diagnosed promptly.
The primary etiologies of internal hemorrhoids are similar to those of hemorrhoidal disease in general, including prolonged standing or sitting and a sedentary lifestyle associated with occupational factors, such as office work, driving, or prolonged static postures.
- Chronic constipation, requiring excessive straining during defecation
- Diarrhea, which may increase the volume and irritation of hemorrhoidal tissue
- Underlying conditions such as irritable bowel syndrome (IBS), increased intra-abdominal pressure, anorectal tumors, or adjacent pelvic masses, all of which elevate the risk of hemorrhoidal disease
- Pregnancy and the postpartum period, due to increased pelvic pressure and hormonal changes
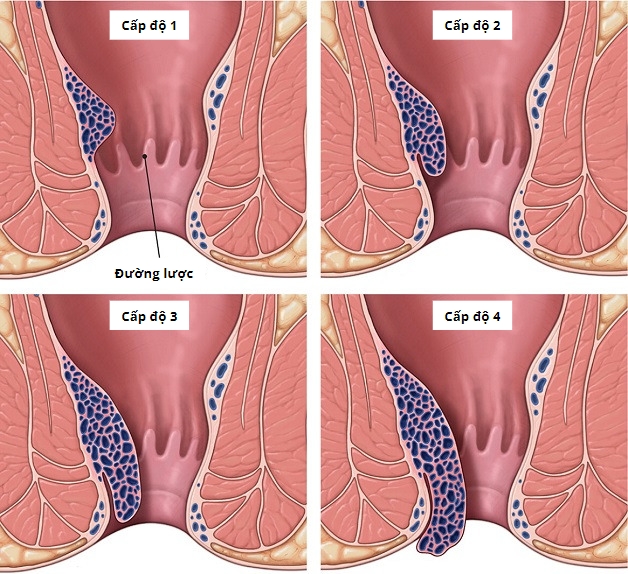
Classification of internal hemorrhoids
Internal hemorrhoids are classified based on clinical manifestations, particularly the degree of prolapse. Accordingly, internal hemorrhoids are divided into four grades as follows:
Grade I internal hemorrhoids
Grade I internal hemorrhoids are characterized by the following clinical features:
- Rectal bleeding during defecation; initially, blood may be noted on the stool or toilet paper, but as the condition progresses, bleeding may increase in volume, presenting as dripping or even spurting during bowel movements
- Anal discomfort, including a burning sensation during defecation and pruritus ani, leading to significant patient discomfort
- Persistent or chronic constipation
At this stage, early recognition and timely intervention are essential. Delayed diagnosis and treatment may result in disease progression, making management more complex and less effective.
Grade II internal hemorrhoids
Clinical manifestations of grade II internal hemorrhoids are more pronounced than in grade I:
- Increased rectal bleeding during defecation
- Anal pain and burning sensation during bowel movements
- Anal pruritus causing discomfort
- Notably, a small prolapsing mass may be observed during defecation; this represents the hemorrhoidal tissue, which typically reduces spontaneously after bowel movement
However, at this stage, due to embarrassment, many patients tend to avoid seeking medical evaluation and instead tolerate the condition. By the time the pain becomes severe, the disease has often progressed, making treatment more complex and less likely to achieve complete resolution.
Grade III internal hemorrhoids
Clinical manifestations of grade III internal hemorrhoids become more pronounced:
- Rectal bleeding may decrease in volume compared to earlier stages
- Hemorrhoidal prolapse occurs and does not reduce spontaneously; manual reduction is required
- Persistent anal pain and burning sensation, even in the absence of defecation; patients may have difficulty sitting due to pressure on the prolapsed hemorrhoidal mass
At this stage, the reduction in bleeding may lead to underestimation of disease severity, causing patients to delay medical evaluation. However, this is considered the last stage at which conservative (non-surgical) treatment may still be effective without the need for surgical intervention.
Grade IV internal hemorrhoids
This represents the most advanced stage of internal hemorrhoidal disease, characterized by:
- Persistent prolapse of hemorrhoidal tissue, even in the absence of defecation
- Irreducible hemorrhoids that cannot be manually repositioned into the anal canal
- Severe pain and bleeding occurring during both movement and rest
At this stage, the condition is associated with a high risk of complications, including:
- Infection and potential necrosis of the prolapsed hemorrhoidal tissue
- Anal fissures and perianal abscess formation
- Increased risk of anorectal malignancy (requiring careful differential diagnosis)
Diagnosis and treatment of internal hemorrhoids by grade
Internal hemorrhoids are classified into four grades, each presenting with varying levels of severity, clinical manifestations, and associated symptoms. Therefore, treatment strategies should be tailored to each grade to ensure optimal outcomes while minimizing time, effort, and healthcare costs.
In general, patients in the early stages (grade I and II) are primarily managed with conservative therapy, including pharmacological treatment and lifestyle modification. In more advanced stages (grade III and IV), medical therapy alone is often insufficient to achieve definitive resolution, and interventional procedures or surgical management may be required.
Reader may also be interested in:
- Signs of internal hemorrhoids and when surgery is indicated
- Prolapsed hemorrhoids: beware of serious complications if not treated promptly
Importantly, patients should undergo a thorough clinical evaluation at a reputable healthcare facility. A detailed assessment by a qualified specialist is essential to determine disease severity and to establish the most appropriate, individualized treatment plan.
Management of grade I and II internal hemorrhoids
Grade I and II internal hemorrhoids represent the early stages of the disease, where hemorrhoidal tissue remains small and symptoms are often mild or nonspecific. As a result, management at these stages is relatively straightforward and primarily involves conservative (non-surgical) treatment.
Patients are typically treated with pharmacological therapy in combination with appropriate dietary modifications and healthy lifestyle habits, including:
- Increasing dietary fiber intake and maintaining adequate hydration; the addition of stool-softening foods and nutrients rich in vitamins, iron, zinc, and magnesium may help improve bowel function and alleviate symptoms
- Avoiding high-fat foods such as fried items and fast food
- Limiting intake of refined carbohydrates, sugars, and alcohol, which may impair digestion and contribute to constipation
- Establishing regular bowel habits with consistent timing each day
- Avoiding prolonged sitting on the toilet and excessive straining during defecation; maintaining proper anal hygiene by gentle cleansing and thorough drying after bowel movements
- Engaging in regular physical activity, rather than prolonged sedentary behavior
These measures aim to reduce straining, improve bowel movements, and prevent disease progression.
Management of grade III and IV internal hemorrhoids
Grade III and IV internal hemorrhoids represent advanced stages of the disease, characterized by enlarged hemorrhoidal masses and progressively worsening symptoms such as pain and discomfort. At these stages, treatment is primarily directed toward definitive removal of hemorrhoidal tissue through interventional or surgical approaches.
Depending on the patient’s clinical condition, physicians will determine the most appropriate modality, including minimally invasive procedures or surgical intervention.
Common surgical and interventional techniques include:
- Laser hemorrhoidectomy: This is an outpatient procedure utilizing focused laser energy to precisely target and ablate hemorrhoidal tissue without the need for a scalpel. The technique allows for rapid removal of hemorrhoids, with reduced postoperative pain and faster recovery time.
- Ferguson hemorrhoidectomy (closed technique): A conventional surgical method in which each hemorrhoidal bundle is excised individually and the wound is sutured. This technique effectively removes hemorrhoidal tissue while preserving the anatomical structure of the anal canal. It is applicable to most cases requiring surgery and demands high surgical expertise and advanced equipment.
- Milligan–Morgan hemorrhoidectomy (open technique): This procedure involves excision of individual hemorrhoidal bundles, leaving bridges of mucocutaneous tissue between the excision sites. In cases of circumferential hemorrhoids, additional hemorrhoidal tissue may be removed. The technique is relatively straightforward, with a short operative time, low recurrence rate (approximately 5–10% over five years), and cost-effectiveness, making it a widely utilized option.
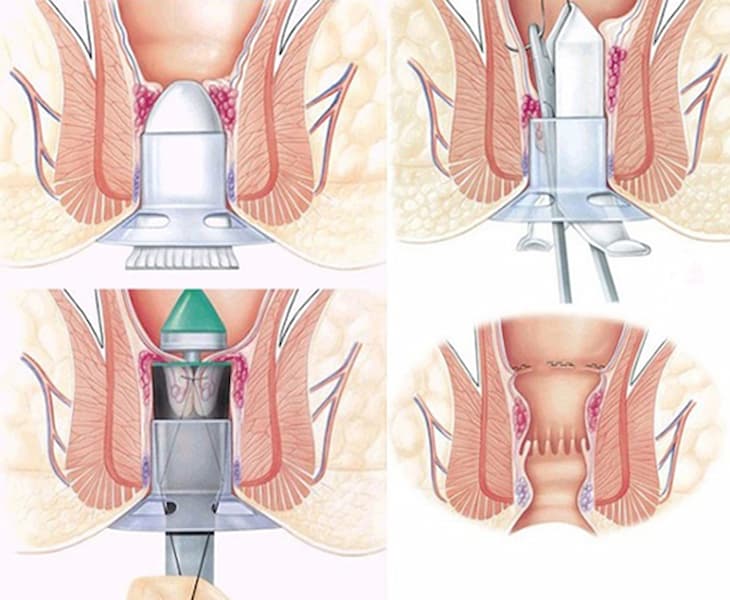
- Longo procedure (stapled hemorrhoidopexy): This technique is based on the principle of repositioning prolapsed hemorrhoidal tissue back to its normal anatomical location. It is commonly indicated for circumferential hemorrhoids or grade III–IV internal hemorrhoids.
The procedure utilizes a circular stapling device specifically designed to excise and staple a ring of rectal mucosa and submucosa above the dentate line (the anatomical junction between the rectum and anal canal, distinguishing internal from external hemorrhoids). This maneuver lifts the prolapsed hemorrhoidal tissue and simultaneously interrupts its arterial blood supply, leading to gradual shrinkage of the hemorrhoids.
This approach is associated with less postoperative pain, faster recovery, and the absence of open wounds or complications such as anal stenosis.
A trusted address for the diagnosis and treatment of internal hemorrhoids
To accurately determine the stage of internal hemorrhoids and identify the most appropriate treatment approach, patients are advised to seek evaluation at reputable healthcare facilities with qualified specialists.
Hong Ngoc General Hospital brings together a highly experienced medical team and a comprehensive system of advanced medical equipment, establishing itself as a trusted destination for patients seeking examination and treatment of hemorrhoidal disease.
Patients can be reassured by the expertise of the Department of Surgery, led by Prof. Nguyen Xuan Hung, MD, PhD, a People’s Physician with extensive experience in colorectal and anorectal disorders.

Prof. Nguyen Xuan Hung, MD, PhD, is one of Vietnam’s leading experts in gastrointestinal surgery and anorectal disorders:
- Former Director of the Colorectal and Pelvic Floor Surgery Center; former Head of the Department of Gastrointestinal Surgery; and former Head of the Outpatient Department at Viet Duc University Hospital
- Vice President of the Vietnam Society of Colorectal and Anal Diseases; member of the Vietnam Society of Surgery and the Vietnam Society of Endoscopic Surgery
- Member of the French Society for the Treatment of Colorectal and Anal Diseases
- Adjunct lecturer at Hanoi Medical University and Vietnam National University, Hanoi
Alongside Meritorious Physician Pham Van Cuong, MD, PhD, Specialist Level II, with nearly 40 years of experience and a member of the Vietnam Society of Endoscopic Surgery and the Vietnam Society of Surgery.
Hemorrhoid treatment with specialists to ensure:
- Accurate diagnosis: avoiding misdiagnosis with rectal cancer, polyps, and other anorectal conditions
- Comprehensive management: approximately 50% of cases can be managed with medication combined with lifestyle and dietary modification, while 45% require only minimally invasive procedures
- Effective intervention: minimal tissue damage, rapid recovery, very low complication rates, with a success rate exceeding 95%
Hotline for appointment booking: (+84) 911 908 856
Hotline for surgical consultation: (+84) 949 646 556
Register to receive information and consultation:
Note: The information provided in this article by Hong Ngoc General Hospital is for reference purposes only and does not replace professional medical diagnosis or treatment. Patients are advised not to self-medicate. For an accurate diagnosis and appropriate treatment plan, individuals should seek direct evaluation by qualified healthcare professionals at medical facilities.
Follow the official fanpage of Hong Ngoc General Hospital for more health information and exclusive programs.