Cardiomyopathy is a serious medical condition affecting a significant number of individuals. If not detected early and managed promptly with appropriate therapeutic interventions, it may lead to severe complications and potentially life threatening outcomes.
What is cardiomyopathy?
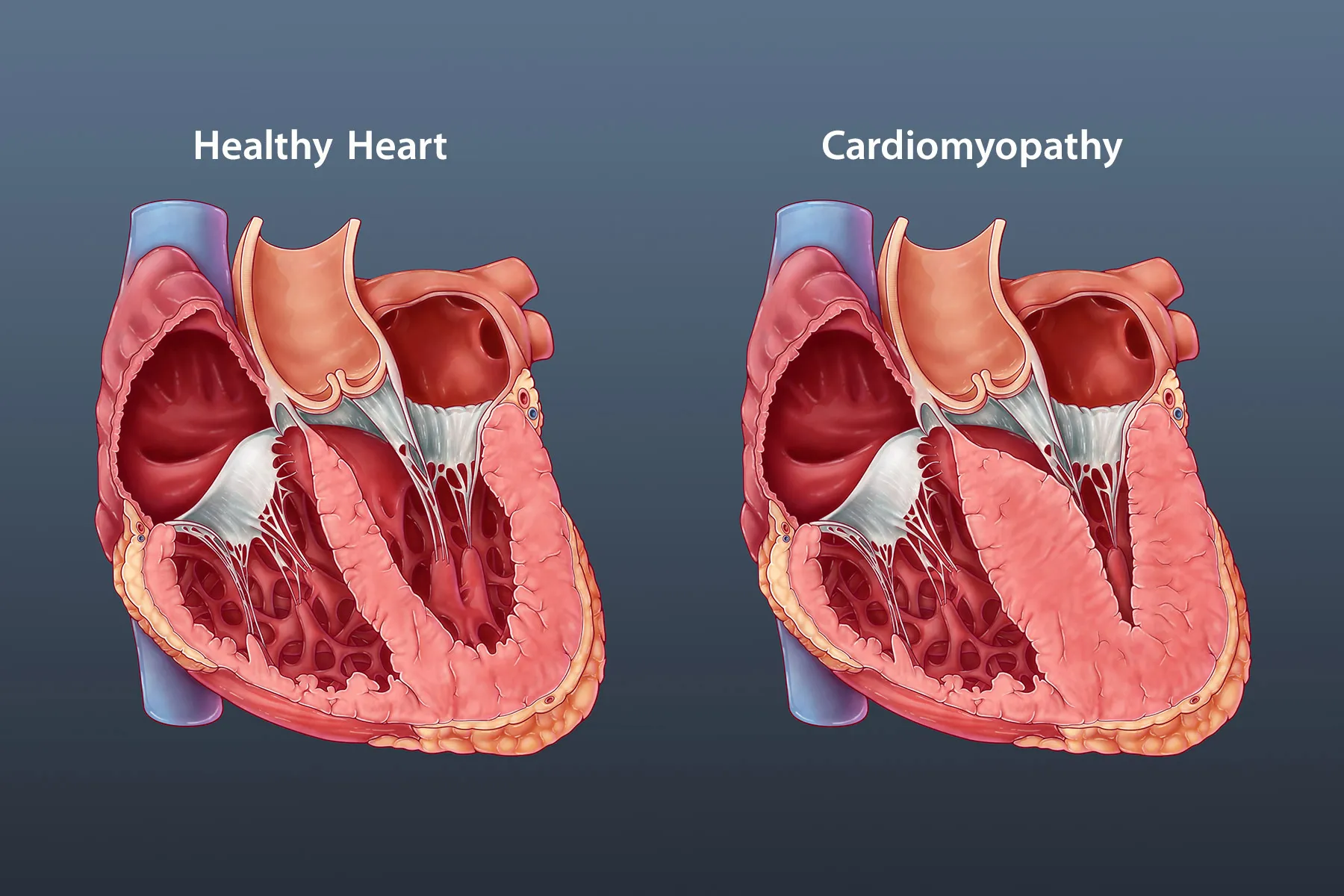
Cardiomyopathy is a broad clinical term referring to diseases of the myocardium that impair the structural integrity and functional performance of the heart muscle. These disorders affect myocardial contractility, relaxation, or both, thereby compromising the heart’s ability to pump blood effectively.
The myocardium plays a central role in maintaining systemic circulation by generating the force necessary to deliver oxygen and essential nutrients to tissues and organs throughout the body. When myocardial function is impaired, cardiac output declines, potentially leading to progressive heart failure and other serious cardiovascular complications.
Common types of cardiomyopathy
Cardiomyopathy encompasses several clinical subtypes. The most frequently encountered forms include the following:
- Dilated cardiomyopathy: A form of myocardial disease characterized by ventricular chamber enlargement and impaired systolic function. In this condition, the left and or right ventricles become dilated, leading to reduced contractility and decreased cardiac output.
- Hypertrophic cardiomyopathy: A disorder in which the myocardium becomes abnormally thickened, most commonly involving the left ventricle. Myocardial hypertrophy may obstruct left ventricular outflow and impair diastolic filling, resulting in compromised intracardiac blood flow.
- Congenital cardiomyopathy: A group of structural or functional myocardial abnormalities present from fetal development. These conditions arise due to abnormal cardiac formation during embryogenesis.
- Stress induced cardiomyopathy: Also known as stress related cardiomyopathy, this is a transient cardiac condition triggered by intense emotional or physical stress. It is characterized by temporary left ventricular dysfunction and reduced myocardial contractility.
- Pericardial disease: Disorders involving the pericardium, including pericarditis and hemopericardium. Although distinct from primary myocardial disease, these conditions may significantly affect cardiac function.
- Secondary cardiomyopathy: Myocardial dysfunction resulting from an underlying systemic disorder, such as metabolic, endocrine, infectious, or autoimmune diseases. In this context, cardiomyopathy represents a complication rather than a primary cardiac pathology.
- Alcoholic cardiomyopathy: A form of dilated cardiomyopathy caused by chronic excessive alcohol consumption, leading to progressive myocardial injury, ventricular dilation, and systolic dysfunction.
Alcohol exerts direct toxic effects on myocardial cells, impairing contractile function and reducing the heart’s pumping capacity. In addition, chronic alcohol exposure may induce myocardial inflammation and structural damage, contributing to progressive ventricular dysfunction.
Causes of cardiomyopathy
Cardiomyopathy may arise from a variety of underlying causes. The most common etiological factors include the following:
Coronary artery obstruction
Coronary artery disease is a major underlying cause of cardiomyopathy. It occurs when the coronary arteries, which supply oxygenated blood to the myocardium, become narrowed or occluded. Atherosclerotic plaque composed of lipids, cholesterol, and inflammatory substances accumulates within the arterial wall, reducing myocardial perfusion. Prolonged ischemia may result in angina pectoris, myocardial infarction, and subsequent ischemic cardiomyopathy.
Hypertension
Chronic elevation of blood pressure imposes sustained hemodynamic stress on the myocardium and vascular walls. Over time, this pressure overload can lead to left ventricular hypertrophy, impaired myocardial relaxation, and progressive cardiac dysfunction. Hypertension is a well established risk factor for heart failure, myocardial infarction, and other cardiovascular complications.
Valvular heart disease
Cardiac valves regulate intracardiac blood flow. Structural or functional abnormalities, such as valvular stenosis or regurgitation, may disrupt normal hemodynamics and increase myocardial workload. Persistent valvular dysfunction can ultimately contribute to ventricular remodeling and cardiomyopathy.
Congenital heart disease
Certain individuals are born with structural cardiac abnormalities affecting myocardial development or intracardiac blood flow. These congenital defects may include septal defects, valvular malformations, or other structural anomalies that impair cardiac function and predispose to cardiomyopathy later in life.

Diabetes mellitus
Individuals with diabetes mellitus have a significantly increased risk of developing cardiomyopathy compared with the general population. Poor glycemic control may lead to microvascular and macrovascular damage, as well as diabetic cardiomyopathy characterized by myocardial fibrosis and impaired ventricular function.
Tobacco use
Active smoking or chronic exposure to secondhand smoke is a major risk factor for cardiomyopathy. Tobacco use damages vascular endothelium, promotes atherosclerotic plaque formation, and increases the risk of myocardial ischemia and infarction affecting the coronary circulation.
Reader may also be interested in:
- 11 Warning signs of heart disease that require immediate medical attention
- Is valvular heart disease life-threatening? Clinical manifestations and contemporary therapeutic approaches
- Valvular regurgitation and therapeutic management
These represent only some of the common etiologies of cardiomyopathy. Additional contributing factors include genetic predisposition, advancing age, coexisting systemic diseases, and unhealthy lifestyle behaviors, all of which may increase susceptibility to myocardial dysfunction.
Clinical manifestations of cardiomyopathy
The clinical presentation of cardiomyopathy varies depending on the specific subtype and severity of myocardial dysfunction. The following are among the most common symptoms observed in affected patients:
Chest pain
Patients may experience angina pectoris, typically described as a sensation of pressure, heaviness, or tightness in the chest. Chest pain often occurs during physical exertion or emotional stress and may be associated with reduced coronary perfusion to the myocardium.
Dyspnea
Shortness of breath is a common manifestation, particularly in patients with heart failure secondary to cardiomyopathy. Dyspnea may occur during exertion, when lying supine, or even at rest in advanced stages, reflecting impaired cardiac output and pulmonary congestion.
Fatigue
Persistent, unexplained fatigue and reduced exercise tolerance are frequently reported. This symptom results from diminished myocardial contractility and inadequate oxygen delivery to peripheral tissues.
Cardiac arrhythmias
Irregular heart rhythms may occur due to electrical instability within the diseased myocardium. Arrhythmias may present as tachycardia, bradycardia, or irregular heartbeat and can increase the risk of adverse cardiovascular events.

Peripheral edema
Cardiomyopathy may lead to fluid retention due to impaired cardiac function and venous congestion. Edema commonly presents in the feet, ankles, or lower legs, and in more advanced cases may involve the hands, face, abdomen, or lungs, as seen in pulmonary congestion.
Cough and wheezing
Patients may experience persistent cough or wheezing, particularly when lying supine. These symptoms are often associated with pulmonary edema secondary to left ventricular dysfunction.
The manifestations described above are among the common clinical features of cardiomyopathy. However, these symptoms are not specific and may occur in various other medical conditions. Individuals experiencing suspicious or persistent symptoms should seek prompt evaluation by a qualified physician for accurate diagnosis and appropriate management.
Diagnosis of cardiomyopathy
The diagnosis of cardiomyopathy is typically established by a cardiology specialist through a comprehensive clinical evaluation combined with targeted diagnostic investigations. The assessment process generally includes the following modalities:
Clinical evaluation and medical history:
The cardiologist will obtain a detailed history of symptoms, past medical conditions, and cardiovascular risk factors. A comprehensive physical examination is performed to assess for signs such as angina, dyspnea, fatigue, peripheral edema, and cardiac rhythm abnormalities.
Laboratory investigations:
Blood tests may include lipid profile assessment such as cholesterol and triglyceride levels, fasting glucose, liver and renal function tests, and inflammatory markers to evaluate systemic involvement and contributing risk factors.
Electrocardiogram (ECG):
An electrocardiogram records the electrical activity of the heart and may detect arrhythmias, chamber hypertrophy, conduction abnormalities, ischemic changes, or other electrical alterations suggestive of myocardial dysfunction.

Cardiac imaging studies:
Imaging modalities such as echocardiography and computed tomography are utilized to evaluate myocardial size, ventricular morphology, valvular structure, coronary arteries, and other intracardiac and extracardiac anatomical features. These techniques provide essential information regarding structural abnormalities and ventricular function.
Functional stress testing:
Exercise stress testing or nuclear stress testing may be performed to assess myocardial perfusion and functional capacity under increased cardiac workload. These investigations help determine the adequacy of coronary blood flow and identify inducible ischemia or exercise related cardiac dysfunction.
Cardiac catheterization and endomyocardial biopsy
- Cardiac catheterization: Cardiac catheterization is an invasive diagnostic and interventional procedure performed under sterile conditions. A thin, flexible catheter is inserted through a peripheral artery, commonly via the radial or femoral approach, and advanced into the cardiac chambers. This technique allows direct measurement of intracardiac pressures, assessment of hemodynamic parameters, and sampling of blood from specific chambers or vessels. In addition, contrast media may be injected to visualize coronary arteries and cardiac structures under fluoroscopic guidance, enabling detailed evaluation of coronary anatomy and valvular function.
- Endomyocardial biopsy: Endomyocardial biopsy is a specialized diagnostic procedure often performed during cardiac catheterization. A small tissue sample of the myocardium is obtained using a biopsy catheter and subsequently analyzed in the laboratory. Histopathological examination can identify myocardial inflammation, fibrosis, infiltrative disorders, or other cellular abnormalities, thereby aiding in the definitive diagnosis of specific types of cardiomyopathy.
Management of cardiomyopathy
Effective management of cardiomyopathy requires accurate identification of the specific subtype and assessment of disease severity to establish an appropriate, individualized treatment strategy.
In general, the standard therapeutic approaches for cardiomyopathy include the following:
- Lifestyle modification: In mild cases of cardiomyopathy, lifestyle changes are very important.
- Maintain a healthy diet rich in fiber and low in cholesterol, and reduce salt and fat intake.
- Exercise regularly with intensity appropriate to individual health status.
- Control body weight and maintain it within a healthy range.
- Limit the use of stimulants such as tobacco and alcohol.
- Medication: Physicians may prescribe medications to treat cardiomyopathy, such as:
- Antihypertensive drugs: Help control blood pressure and reduce the risk of heart failure.
- Cholesterol lowering drugs: Help control blood cholesterol levels and reduce the risk of coronary artery obstruction.
- Antianginal medications: Help relieve chest pain and improve blood flow to the myocardium.
- Analgesic and anti inflammatory drugs: Used to relieve inflammation and pain in cases of myocarditis.
- Surgery: In some severe cases, patients may be indicated for surgical treatment. Surgical options may include:
- Valve replacement: Replacing a damaged or malfunctioning heart valve with a prosthetic valve.
- Plaque removal: Surgical removal of atherosclerotic plaques within the coronary arteries.
- Vascular grafting: Use of a vascular graft to restore blood supply to the myocardium. This procedure is commonly performed in cases of severe coronary artery disease.
- Supportive therapy: In addition, supportive measures such as periodic medical follow up, nutritional counseling, and individualized exercise programs are implemented to support treatment and improve the patient’s quality of life.
Management of cardiomyopathy must be prescribed and closely monitored by a cardiology specialist. Each patient requires an individualized treatment regimen based on specific clinical characteristics and disease severity. Patients should not self medicate or adopt another individual’s treatment protocol without professional medical evaluation and supervision.
When diagnosed with cardiovascular disease, patients should seek evaluation at a reputable cardiology department for comprehensive assessment, specialized diagnostic testing, and an individualized treatment plan prescribed by qualified cardiology specialists.

The Cardiology Department at Hong Ngoc General Hospital is a trusted destination for comprehensive cardiovascular care. With a highly qualified team of cardiologists and advanced diagnostic equipment, the department enables early detection of cardiomyopathy and provides individualized, evidence based treatment strategies tailored to each patient’s clinical condition.
Register for a consultation with our Cardiology specialists here:
Note: The information provided in this article by Hong Ngoc General Hospital is for reference purposes only and does not substitute for professional medical diagnosis or treatment. Patients should not self medicate or independently purchase medications without medical supervision. For an accurate evaluation of any medical condition, individuals are advised to seek direct consultation at a healthcare facility for comprehensive examination, definitive diagnosis, and appropriate therapeutic guidance from qualified physicians.
Follow the official fanpage of Hong Ngoc General Hospital for more reliable health information and medical updates.